


I was in a Facebook group the other day and came across a woman who was recommended a hysterectomy for heavy bleeding.
Before I decide whether to respond, I often read a few comments first to see what other women are saying. Personally, I think a hysterectomy is rather extreme but there were a few ladies who were saying their hysterectomy “was the best thing they have done.”
Now, this is not the first time I am seeing comments like this, but its so common I am starting to get a little miffed For me personally, its incredibly jarring and almost feels like an orchestrated push. But of course, I have no way of knowing that for sure, however, I do fully lean into my gut feelings, which is never wrong. But let me put my thoughts and feelings to one side, take a big step back and look at this with an unbiased lens.
Having been in many groups over the last eight years, it’s clear to me how widespread the ignorance is around women’s bodies and anatomy - and I include myself in that. When I say ‘ignorance,’ I don’t mean it as a dig; it’s simply a gap in what we’ve all been taught. The narrative that has been pushed on all of us – as in what we were taught, is that your uterus is nothing more than a baby bag. You are lead to believe that its disposable. What do I mean by that? If you have fibroids for example, the question your gynae likes to ask is “are you done having children?”, like your womb is some major inconvenience and your life will be much better without it. That is the preconception pushed on to us as women. The truth is, your womb does so much more than carry babies.
Your uterus plays a major role beyond carrying children and this is what many of us as women might not be aware of. In my groups, I meet women who’ve learned this only after the fact - often too late. If you’re being offered a hysterectomy or it’s been suggested, it’s vital to understand how this organ truly functions.
Your uterus plays a vital role in structural pelvic support, hormone communication with the ovaries, and sexual function. It is a vital organ, and minimising it down to nothing more than a temporary container is a huge disservice to women’s health. And I need to address the notion of a hysterectomy being the “best thing I ever did.” This usually comes down to two major factors:
Desperation and Relief
Women who join fibroid groups are more often than not, dealing with severe, life-altering symptoms. I am talking about bleeding so heavily they cannot leave the house, fatigue beyond fatigue, chronic anaemia, and agonising pain. When someone goes from that level of suffering to suddenly having their life back, the relief is so massive that they want to shout it from the rooftops. I get totally get that. Its no different if I had found a miracle cure that obliterated fibroids. I’d be shouting that from the rooftops as well!
The Vocal Minority
Women who have a hysterectomy and experience no complications are more likely to post positive reviews. On the other hand, women who managed their fibroids naturally, had a successful minor procedure (like a myomectomy), or had a bad hysterectomy experience might be in entirely different sub-groups or have moved on with their lives, so this creates an echo chamber where major surgery looks like the default happy ending.
My frustration stems from the lack of informed consent, which is sorely lacking, and let’s not sugar coat this: a hysterectomy is major abdominal surgery, and while it maybe a necessary, lifesaving, or sanity-saving choice for many women, there is no denying the long-term risks that you need to be aware of before making a decision.
To help balance the narrative, let me show you what the uterus does beyond childbearing. I’ll also share the genuine risks that are often left out of the “best decision ever” comment I come across all the time.
The Uterus Beyond Pregnancy
Pelvic Structural Support: Your uterus is held in place by a complex web of ligaments and tissues. It acts as a structural anchor for your pelvic floor, helping to keep your bladder and bowel properly positioned.
Ovarian Blood Supply: The uterine artery provides a significant portion of the blood flow to your ovaries. Even if you keep your ovaries during a hysterectomy, disrupting this blood supply can sometimes cause the ovaries to fail, sending a woman into premature menopause.
Anatomical Sexual Function: For many women, uterine contractions are a key component of orgasms, and the cervix plays a structural role in the mapping of the vaginal canal.
Potential Long-Term Consequences of a Hysterectomy
You might want to spend time researching the following:
Pelvic Floor Health
There is an increased long-term risk of pelvic organ prolapse (bladder or bowel dropping) due to the removal of the central support structure.
Cardiovascular & Bone Health
If ovarian function drops or menopause is induced early, the risk of heart disease and osteoporosis (bone thinning) increases significantly.
Urinary Incontinence
Damage to surrounding nerves or the shifting of pelvic organs can sometimes lead to bladder control issues sooner or later.
Less invasive options for fibroids do exist, like Uterine Artery Embolisation (UAE), MRI-guided ultrasound, or targeted myomectomy (removing just the fibroids). Just know, there is a chance UFE might fail. Over a decade, about 35% (roughly 1 in 3) of women who had UFE ended up getting a secondary hysterectomy, usually because their symptoms returned or new fibroids grew, so its best to bear this in mind when you are doing your research or learning more about different procedures.
I also must point out the following about UFE:
1. It does not eliminate the cause of fibroids: UFE works by cutting off the blood supply to existing fibroids, causing them to shrink by about 40% to 60%. It kills the current tumours, but it does not change the underlying factors that caused their growth. If your body is prone to making fibroids, new ones can grow years down the road. But you aware of that anyway.
2. The “Re-intervention” Trap: Interventional radiologists consider UFE a success if it buys a woman 5 to 7 years of symptom relief until she hits menopause (when fibroids naturally shrink). But to a patient, having to go back for a second procedure or a hysterectomy 5 years later feels like a flat-out failure of the first attempt.
3. Poor Patient Selection: UFE is frequently offered to women who are bad candidates for it. Let me explain: if you have a massively enlarged uterus, an extremely large dominant fibroid (greater than 10 cm), or certain types of pedunculated fibroids (hanging by a stalk), UFE has a much higher rate of complications or failure. When doctors push UFE as a blanket alternative without strict screening, it leads to higher rates of further surgery.
The Trade-Off
Ultimately, it highlights a frustrating compromise we, as women are forced to make:
The choice tends to boil down to:
Do you want a 100% definitive, one-and-done cure that guarantees the fibroids can never return, but requires losing a vital organ (Hysterectomy)?
Or do you want a minimally invasive, 1-week recovery that preserves your body’s anatomy, but carries a 35% chance you might need surgery down the road anyway (UFE)?
It’s completely fair to look at that 1-in-3 chance of eventually needing a hysterectomy and decide UFE isn’t worth the risk or the recovery time. Every woman’s threshold for that gamble is different, which is why transparency is crucial. Personally, I did tons of research before I made a decision to have surgery, but at the time my options were limited to myomectomy or hysterectomy. Well, that is what I was told.
Further, it’s super important to keep pushing back against the idea that a hysterectomy is a quick fix without consequences. You deserve to know the full picture. The highlights of an online support group is not enough for you to make such a major decision.
It took me four years to make the decision to have surgery (myomectomy). For me, it was a major decision, second, I needed to ensure it was the right way to go and third, I needed to trust my gut when it came to choosing a gynaecologist. I did not just except what the first guy said – besides, I did not like his ‘attitude’. It’s my body, so it was my choice. I had to feel confident that when I went under the knife, I would wake up with my uterus intact, so the only way I could ensure this was to say I wanted to start a family. He wrote hysterectomy on my consent form as a ‘just in case’. Really? I reluctantly signed the form and trusted in Divine Wisdom to keep me safe.
When you make the decision to have a hysterectomy, rarely are you told about the long term implications of removing your uterus. I began looking more deeply into this because when I look back to my experience, my gut was telling me to keep my womb despite the suffering I was going through. Many women have similar strong feelings but override or justify their decision because of their suffering, but its only fair you know the health issues a hysterectomy could potentially cause later down the line.
The Heart and Bone Connection
When your uterus is removed, it affects fertility and alters your endocrine (hormonal) environment and vascular anatomy. The research shows significant long-term risks, even when your ovaries are left behind.
Cardiovascular Health (Heart Disease)
For decades, women were told that keeping their ovaries during a hysterectomy meant their hormones—and therefore their heart health—would remain perfectly intact. Landmark studies have proven this is not entirely true.
The Mayo Clinic Cohort Study (ROCHESTER Epidemiology Project): This massive study tracked over 2,000 women who underwent a hysterectomy with ovarian preservation (meaning they kept their ovaries) and compared them to a control group of intact women.
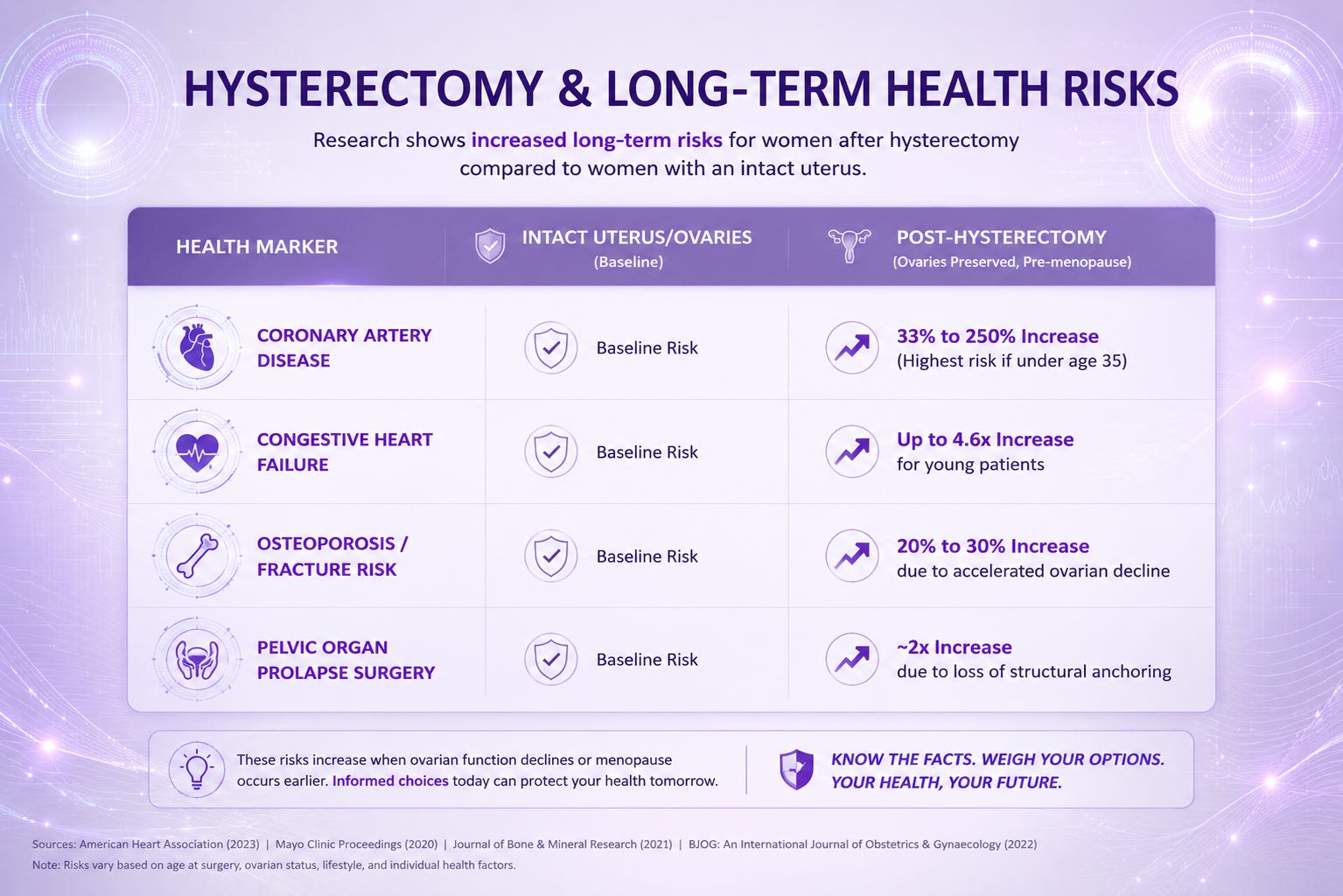
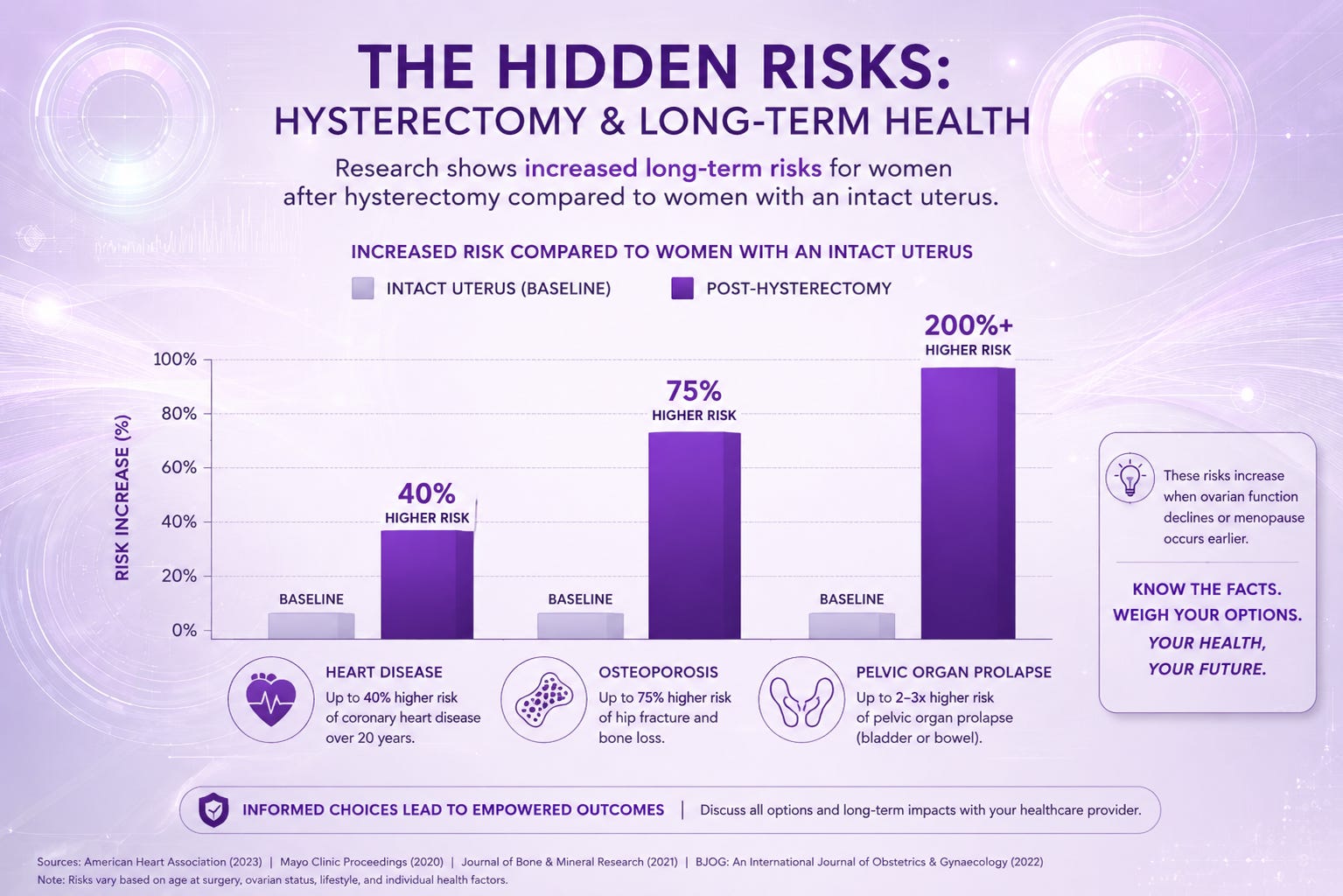
The Findings: Women who had a hysterectomy before age 35 experienced a 4.6-fold (460%) increased risk of congestive heart failure and a 2.5-fold (250%) increased risk of coronary artery disease over their lifetime. Even for women undergoing the procedure at a typical age (under 50), there was a 33% increased risk of coronary artery disease.
Why does this happen? The uterine artery provides a massive portion of the collateral blood supply to the ovaries. When the uterus is removed, that blood supply is disrupted. The ovaries don’t always die immediately, but they experience ovarian insufficiency, meaning they stop producing optimal levels of oestrogen, progesterone, and testosterone years earlier than they naturally would have. Oestrogen is highly protective of blood vessels; when it drops, cardiovascular risk spikes.
Skeletal Health (Osteoporosis and Fractures)
Bone health is intimately tied to ovarian function, and because hysterectomy frequently accelerates ovarian decline, it directly impacts bone density.
Bone Loss: Long-term observational studies show that women who undergo a hysterectomy, even while keeping their ovaries, experience significantly higher rates of bone mineral density (BMD) loss compared to age-matched women who kept their uterus.
Increased Fracture Risk: Research published in journals like Osteoporosis International indicates that women who have a hysterectomy face a roughly 20% to 30% higher risk of developing osteoporosis and experiencing bone fractures (particularly in the spine and hip) later in life.
The Mechanism: Bone is a dynamic tissue that is constantly breaking down and rebuilding. Oestrogen regulates the cells that break down bone (osteoclasts). Without the precise, cyclical hormone signalling managed by the uterine-ovarian axis, bones breakdown faster than they can be replaced.
Structural and Neurological Impact
Beyond hormones, the physical absence of your uterus changes the internal mechanics of your body.
Pelvic Organ Prolapse (POP): A large-scale study utilising data from the Swedish National Health Registers tracked over 160,000 women. It found that women who had a hysterectomy were nearly twice as likely (1.9 times) to undergo surgery for pelvic organ prolapse later in life compared to women who hadn’t had the procedure. The risk is highest in the 5 to 10 years following the surgery because the central support structure anchoring the bladder and bowel is gone.
Autonomic Nerve Disruption: The uterus is surrounded by a dense network of nerves (the pelvic plexus) that sends signals to the bladder, bowel, and sexual organs. Disruption of these nerves during surgery is why long-term studies show an increased incidence of urinary incontinence and faecal urgency or constipation post-hysterectomy.
A quick comparison of long-term health risks between women with an intact uterus and those post-hysterectomy (ovaries preserved, pre-menopause):
Moving Forward
There is a growing number of women who are looking toward uterine preservation and thankfully, gynaecology is slowly catching up. Further, more and more data is showing that your uterus has systemic value pre and post birth. It is an endocrine organ and a structural anchor.
When people think of the uterus as nothing more than a baby bag, they are displaying a lack of anatomical literacy. A man’s prostate isn’t called a semen bag and routinely removed the moment he is done having children, because medicine recognises its structural and hormonal importance. Your uterus deserves the exact same medical respect.
Now that you have the facts on your side, take a close look at the long-term data, and trust your instincts.
P.S. It might help to watch this video on the Female Anatomy before making your final decision. You will learn more about your body in 11 minutes than all those years you spent at school.
Disclaimer
This article is for informational and educational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this article.
I am not a medical professional, and the information shared here is based on personal experiences, two decades of knowledge on working on myself, the many brilliant teachers who have taught me everything I know; but most of all and the most important is the insights from my clients, and I fully acknowledge that hysterectomy is a necessary, life-saving, and sanity-saving tool for many women with extreme disease.