


If you read last week’s piece, The Reality of Hysterectomy, you already know that the uterus is far more than a holding container for babies. You learned about its role in pelvic support, its critical connection to ovarian blood flow, and the long-term risks to your heart and bones that rarely, if ever gets mentioned during consent discussions.
But there is more!
While we were discussing structural support and heart health, an equally shocking revolution has been happening in the medical literature. Hold on to your seat! You might not yet be aware of this but the medical community has been publishing massive, multi-million-patient studies that completely rewrite what we know about the uterus. For decades, a woman’s uterus was viewed as an inert muscle sack, useless once childbearing is done. Charming right?
Today, modern endocrinology and gynaecology view it as an (get this), active participant in a woman’s metabolic, signalling, and even cellular ageing pathways.
If you are considering a hysterectomy, or you’ve already had one and are wondering why you feel different, you need to know this data. It’s the missing piece of the puzzle.
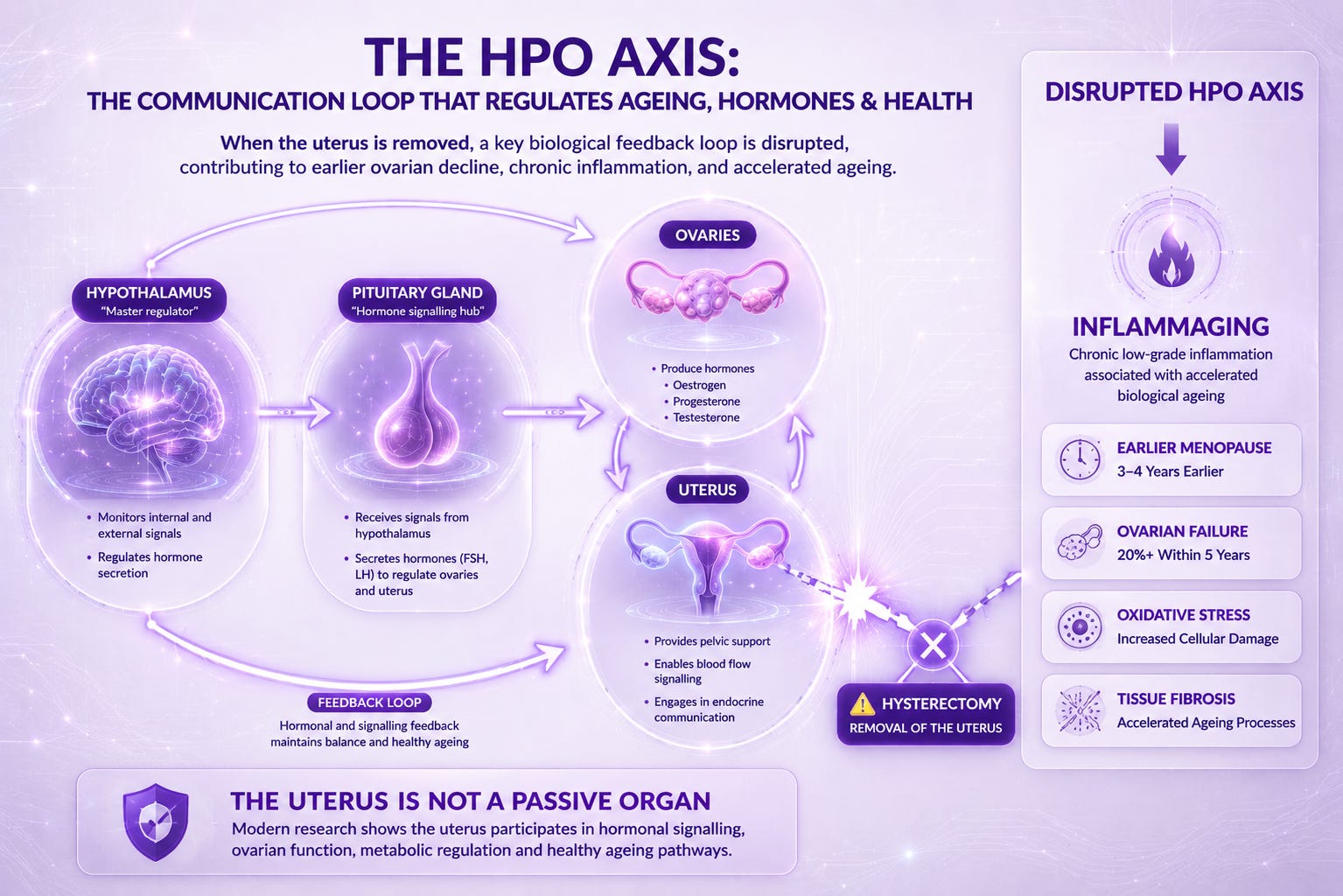
The Inflammaging Effect: Why You Age Faster
One of the most profound findings in recent research is how a hysterectomy accelerates systemic ageing. We’ve just been told our hormones are decreasing, but its so much more than that. The biological alarm bell is literally going off.
The Mechanism
Your uterus and ovaries communicate via a delicate feedback loop called the hypothalamic-pituitary-ovarian (HPO) axis. When the uterus is removed, this entire communication network is severed.
This sudden disruption triggers chronic, low-grade systemic inflammation. Researchers call this inflammaging. It induces massive cellular oxidative stress and tissue fibrosis throughout the body.
Because of this inflammatory response and the disrupted blood supply, women who keep their ovaries during a hysterectomy still enter menopause 3 to 4 years earlier than women who keep their uterus. Within just 5 years of the surgery, more than 20% of women experience complete ovarian failure. In other words, your body clock was reset prematurely.
Metabolic Syndrome: The Diabetes Connection
For years, the focus on was heart health. But the latest large-scale cohort studies (published as recently as 2026) have shifted the focus to cardiometabolic health.
A large study looking specifically at women with fibroids found that those who had a hysterectomy had significantly higher odds of developing:
Type II Diabetes (20% increased risk)
Hyperlipidemia / High Cholesterol (14% to 26% increased risk)
Hypertension / High Blood Pressure
Why? The research proves your uterus participates in active vascular and metabolic signalling. When it’s removed, your body’s ability to regulate fat metabolism and insulin sensitivity changes - independent of whether the ovaries are kept. This means even if you keep your ovaries, you are still at a higher risk for metabolic disorders simply because the organ that helps regulate them is gone.
Brain Health: The Silent Risk
This is perhaps the most heavily guarded piece of data in women’s health. For years, women were told that removing the uterus had zero effect on the brain – and that is if you were told anything about that at all. Neurology journals are now proving otherwise.
Epidemiological data tracking long-term outcomes noted a stark rise in cognitive decline following the removal of reproductive organs. It is estimated that up to 100,000 cases of dementia per year may be directly attributed to surgical removal of the ovaries (often done during hysterectomies).
Furthermore, a massive study involving 2.9 million participants confirmed that a hysterectomy significantly increases a woman’s lifetime risk of suffering a stroke, particularly when the procedure is done pre-menopause.
Read that again. Almost 3 million participants.
What About UFE? The Flip Side of the Research
In Part 1, I mentioned Uterine Fibroid Embolisation (UFE) as a less invasive alternative, but noted the 35% chance of needing further surgery. Now, we need to look at the specific risks to the ovaries that are never tend to get mentioned:
The Ovarian Bypass Risk: The uterine artery and the ovarian artery are closely connected by a network of tiny blood vessels (collaterals). When an interventional radiologist injects embolic particles to starve a fibroid, those particles can sometimes accidentally travel down these collateral pathways and block the blood supply to the ovaries.
The Ovarian Reserve Drop: Modern testing tracks this using Anti-Müllerian Hormone (AMH) levels, which measure egg supply. Studies show that after UFE, women often experience a transient drop in AMH levels within the first 3 months due to this accidental particle drift.
The Silver Lining (and the Catch): Unlike a hysterectomy, where the tissue is gone forever, your ovaries are highly resilient. In most younger women, your body recruits backup blood supply, and AMH levels completely recover by 6 to 12 months post-procedure.
However, for women over 45 who are already close to menopause, that temporary hit can be enough to push the ovaries into permanent retirement. This ties directly back to my point in the last article: the 1-in-3 risk isn’t only about fibroids returning; it’s also about whether your body can recover from the insult of the procedure.
Armed with the Facts
The next time someone tells you the uterus is just a baby bag, you can confidently correct them with the weight of millions of patients’ data behind you. You can confidently say that:
The uterus is actively involved in metabolic signalling. Removing it increases a woman’s long-term risk of type 2 diabetes, high cholesterol, and stroke, and it triggers chronic inflammation that sends her into menopause years ahead of schedule, even if she keeps her ovaries.
Education is sorely lacking and gynaecology has a long, paternalistic history of treating women’s reproductive organs as disposable components once childbearing is complete. The science has evolved past this ‘old boys’ way of thinking; it’s time for standard medical conversations to catch up.
You deserve to know the full picture and the long-term cost.
Disclaimer
This article is for informational and educational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this article.
I am not a medical professional, and the information shared here is based on personal experiences, two decades of knowledge on working on myself, the many brilliant teachers who have taught me everything I know; but most of all and the most important is the insights from my clients. I fully acknowledge that the decision to have a hysterectomy is an emotional one. The intention with these articles is to help fill the gap with vital information that is currently lacking during a consultation.
Thank you so much for all your insightful articles. You truly make a difference!